



The Doctor Will (Maybe) Kill You Now

We’re a society obsessed with spectacular ways to die. We fret about shark attacks, plane crashes, and rogue asteroids, yet we blissfully ignore the far more probable threat lurking in the sterile, brightly-lit hallways of our healthcare system.
The inconvenient, darkly humorous truth is that one of the leading causes of death in the United States is the medical care intended to save you [citation: 2] [citation: 5]. It's a phenomenon called "iatrogenesis"—a fancy Greek term for "brought forth by the healer," which is a polite way of saying your treatment was a success, but the patient died.

Key Points:
* A Hidden Epidemic: While not officially listed on death certificates, peer-reviewed analyses estimate that preventable medical errors cause approximately 251,000 deaths in the U.S. annually, which would make it the third-leading cause of death [citation: 5]. Some studies, accounting for underreporting, push this figure as high as 440,000 [citation: 3].
* Putting It in Perspective: To grasp the scale, consider the numbers from 2023. Medical errors (≈251,000) killed more than twice as many people as drug overdoses (105,000+) and nearly six times as many as motor vehicle accidents (43,273) combined [citation: 2] [citation: 3].
* It's Not Just Mistakes: Iatrogenic harm isn't limited to a slip of the scalpel. It includes everything from adverse drug reactions to properly prescribed medications—which kill over 100,000 people a year—to the systemic over-prescription of drugs like statins, a topic we'll dissect with surgical imprecision later on.
This isn't a screed against doctors and nurses, most of whom are dedicated professionals trapped in a flawed system. Instead, it's an exploration of a massive, under-recognised public health crisis. I'll dive into the data, question the conventional wisdom on treatments like statins, and ask why a problem that kills more people than guns, cars, and opioids combined gets so little attention.
Statistics: A Grim Reality
If you’re looking for a new, statistically-backed existential fear, put away the shark documentaries and turn your gaze to the nearest hospital. The data on iatrogenic harm—death by medical care—is staggering enough to make you consider treating your next ailment with crystals and a positive attitude. While official tallies are notoriously slippery, the numbers painted by researchers are grimly impressive.
The Unofficial Heavyweight Champion of Causes of Death
The central, jaw-dropping claim comes from a landmark 2016 Johns Hopkins analysis, which estimated that preventable medical errors kill approximately 251,454 people in the U.S. each year [citation: 5] [citation: 10]. This figure would comfortably place medical errors as the third-leading cause of death, right behind heart disease and cancer [citation: 1] [citation: 5]. Some analyses, accounting for the systemic underreporting on death certificates, push this estimate even higher, to a terrifying 440,000 annual deaths [citation: 3] [citation: 4].
The reason you don't see "Oops, my bad" on the CDC's official list of mortality causes is that "medical error" lacks a specific International Classification of Disease (ICD) code [citation: 6]. This forces researchers to rely on retrospective studies and chart reviews, leading to a debate over the exact numbers, though even conservative estimates are alarming [citation: 4]. Critics argue the methodology is flawed, but even lower-end estimates from other countries suggest tens of thousands of preventable deaths annually, a far cry from zero [citation: 1] [citation: 4].
To put this in perspective, let's compare it to the things we're actually told to worry about.
Annual U.S. Deaths: A Morbid Scorecard (2023 Data)

As the table shows, your annual check-up is statistically more dangerous than a cross-country road trip with a trunk full of fentanyl. Medical errors claim more than double the lives lost to the opioid crisis and nearly six times the number of traffic fatalities combined [citation: 2] [citation: 3] .
Trends and Disparities: An Equal-Opportunity Disaster?
While the overall picture is bleak, the data reveals interesting and disturbing trends when broken down.
A Tale of Two Trends:
Analysis of CDC WONDER data shows a complicated history. The mortality rate for "medical misadventure" actually *declined* significantly between 1999 and 2020 [citation: 14: Finding 1]. However, a different analysis focusing on broader "iatrogenic error–related mortality" found that, after years of decline, rates increased by 17.2% between 2015 and 2020, with an even sharper 18.4% increase for adults aged 65 and older [citation: 14, Finding 1].
Demographic Divides:
The risk isn't distributed equally. Non-Hispanic Black individuals have the highest age-adjusted mortality rate from medical misadventure, while women have a slightly higher rate than men [citation: 14: Finding 1].
Geographic Hotspots:
Where you live matters. In 2020, Mississippi had the highest iatrogenic error mortality rate at 10.43 per 100,000, while Massachusetts had the lowest at 4.45 per 100,000 [citation: 14: Finding 1].
This data paints a picture of a massive, silent epidemic. It's a problem that, despite its scale, remains largely invisible in public discourse and official statistics, all while costing the nation an estimated $20 billion to $45 billion annually in preventable harm [citation: 2] [citation: 14: Finding 1].
The Prescription Dilemma
If you thought the most dangerous part of the healthcare system was a surgeon who got a C- in medical school, allow me to introduce you to the humble prescription pad. It turns out that the pen—or, more accurately, the e-prescription sent to CVS—is mightier than the scalpel, and far more prolific in its unintended consequences. The world of prescription drugs is a minefield of preventable harm, neatly divided into two terrifying categories: drugs that kill you even when taken correctly, and drugs that kill you because someone messed up.
Two Paths to Pharmaceutical Peril
Understanding the prescription dilemma requires separating two distinct, yet equally alarming, problems: Adverse Drug Reactions (ADRs) and outright medication errors.
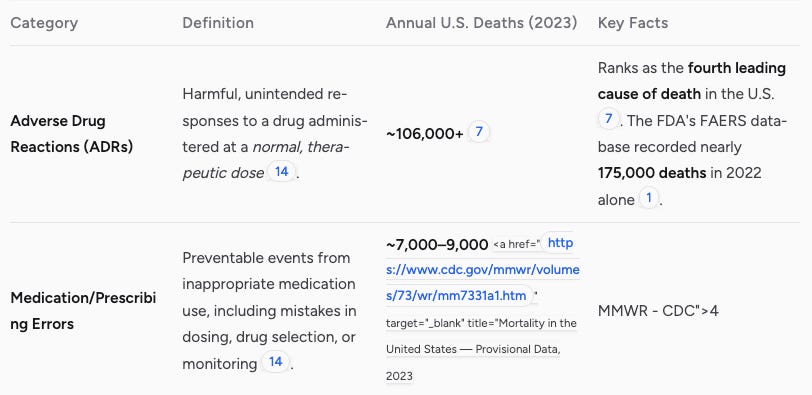
The data is stark: you are overwhelmingly more likely to be killed by a drug that was prescribed *correctly* than by one prescribed by mistake. While medication errors are a serious problem, with nearly half occurring at the prescribing stage, they are dwarfed by the sheer scale of deaths from ADRs [citation: 5]. This raises a deeply uncomfortable question: if the "right" drug at the "right" dose is the fourth leading cause of death, what does that say about our approach to medication?
Case Study in Controversy: The Statin Situation
No drug illustrates this dilemma better than statins. Hailed as a miracle for cardiovascular disease prevention, statins are also at the center of a fierce debate about over-prescription and iatrogenic harm [citation: 13].
The Benefit vs. Harm Debate
Critics argue that the benefits of statins, particularly for primary prevention in low-risk individuals, are wildly overstated [citation: 1]. The issue often boils down to a statistical sleight of hand:
Relative vs. Absolute Risk:
Mainstream reports often highlight a relative risk reduction, which sounds impressive. However, the absolute risk reduction is often minuscule, with analyses showing it can be under 1-2 percentage points [citation: 13]. This means hundreds of people need to be treated for just a few to avoid a heart attack, a trade-off that becomes questionable when considering the side effects [citation: 4].
Under-Recognised Harms:
The potential for iatrogenic harm is significant. Up to 29% of patients report muscle-related issues (myotoxicity), a modest but real risk of new-onset diabetes exists (about one extra case per 1,000 patient-years), and rare but serious liver injury is documented [citation: 2].
A System Primed for Over-Prescription
Many healthcare professionals voice concern that prescribing guidelines are too broad, leading to unnecessary treatment, especially in older adults [citation: 1] [citation: 5]. The American College of Cardiology and American Heart Association guidelines have been criticised for using risk calculators that may qualify millions for statin therapy without a clear, substantial benefit [citation: 1] [citation: 5]. This creates a system where the default is to medicate, often without a thorough discussion of the modest absolute benefits versus the potential for lifelong side effects [citation: 9].

Potential Paths Forward
Addressing this prescription dilemma isn't about abandoning valuable medications but about adopting a more cautious and personalised approach.
System-Level Fixes:
For medication errors, implementing technologies like Computerised Provider Order Entry (CPOE) has been shown to reduce prescribing mistakes by over 50% [citation: 5].
Personalised Medicine:
For ADRs, the future may lie in pharmacogenomic testing. This involves analyzing a patient's genes to predict their response to a specific drug, potentially avoiding life-threatening reactions before the first pill is even swallowed [citation: 3] [citation: 5].
Informed Consent:
Ultimately, a cultural shift is needed toward transparent, shared decision-making where patients are given the absolute risk numbers, not just the relative ones, allowing them to weigh the actual benefits against the real risks [citation: 9] [citation: 13].
The Systemic Issue
It’s tempting to picture medical errors as the fault of a lone, bumbling surgeon who confuses a kidney with a spleen. The reality is far more mundane and systemic. The staggering number of iatrogenic deaths isn't primarily caused by bad doctors, but by a convoluted, poorly designed system that sets up good people to fail [citation: 5]. This system is plagued by flawed incentives, broken reporting mechanisms, and clinical guidelines that can encourage overtreatment.
The Black Hole of Data: If a Death Isn't Coded, Does It Count?
One of the most profound systemic failures is the inability to even track the problem accurately. The reason medical error isn't listed as the third-leading cause of death by the CDC is embarrassingly simple: there is no official billing code for it [citation: 6].
The ICD Code Gap:
Death certificates rely on the International Classification of Diseases (ICD) codes to list a cause of death. You can die from "Contact with venomous spiders" (X21) or "Forced landing of spacecraft injuring occupant" (V95.43), but there’s no code for "Fatal dosage miscalculation."
Consequences of Invisibility:
This glaring omission forces researchers into the complex, debated world of retrospective analysis and extrapolation from small studies [citation: 3] [citation: 4]. It keeps the problem out of official mortality statistics, shielding it from public pressure and policy focus. Dr. Martin Makary, who led the Johns Hopkins study, has explicitly argued for a change in how the CDC collects this data to make the problem visible [citation: 5].
Flawed Guidelines and the Tyranny of Relative Risk
The system often pushes healthcare providers toward overtreatment through flawed clinical guidelines and misleading statistics. The controversy surrounding statins serves as a perfect case study in how systemic incentives can lead to widespread potential harm [citation: 13].
Overstated Benefits:
Many clinical trials and pharmaceutical marketing materials emphasize relative risk reduction, which can make a drug's benefit seem enormous. However, the absolute risk reduction is often minuscule, sometimes under two percentage points [citation: 6] [citation: 13: Finding 4]. This statistical framing can mislead both doctors and patients into believing a treatment is more effective than it truly is, encouraging prescriptions where the potential for iatrogenic harm outweighs the modest benefit [citation: 11: Finding 2].
Broad and Questionable Guidelines:
Critics argue that guidelines from major bodies like the American Heart Association are too broad, recommending statins for huge swaths of the population, including low-risk and older adults, where the evidence for net benefit is weak [citation: 12: Finding 5] [citation: 12: Finding 2]. This creates a default-to-prescribe culture, shifting the focus from personalized care to checking a box on a guideline.
A Culture of Silence and Insufficient Accountability
Beyond flawed data and guidelines, the healthcare system struggles with a deeply ingrained lack of transparency and accountability.
Underreporting is Rampant:
Studies suggest that less than 10% of all medical errors are ever reported [citation: 5]. This isn't just about avoiding lawsuits; the psychological burden on healthcare professionals who make a mistake can be immense, discouraging them from coming forward in a system that often seeks individual blame over systemic solutions [citation: 8: Finding 2].
Lack of Systemic Learning:
Without robust reporting, there is no opportunity for systemic learning. The Joint Commission mandates a "root cause analysis" for major errors, but if the vast majority of errors go unreported, the system cannot identify and fix the underlying processes that led to the mistake in the first place [citation: 2]. This ensures that the same types of errors are repeated across different hospitals and clinics.

To truly address iatrogenic harm, the focus must shift from blaming individuals to redesigning the systems that facilitate these errors. This includes mandating better data collection, promoting transparency in reporting both risks and benefits, and fostering a culture where safety and patient-centered outcomes are valued above procedural compliance.
SUMMING UP
Finally I will discuss CPOE systems [citation: 5] and pharmacogenomic testing [citation: 3] [citation: 5] as concrete examples of tech-driven solutions. I'll also touch on deprescribing and comprehensive medication reviews to counter polypharmacy risks [citation: 4].
Sidebar Regarding The Tone Of This Article:
The tone, I hope, will remain humorous and a bit cynical, but the solutions will be presented as practical and serious.
Strategies for Safer Healthcare
After staring into the abyss of iatrogenic harm, it’s easy to conclude that the safest healthcare strategy is to live in a bubble and subsist on kale. But since that’s impractical, wrong and joyless, the alternative is to fix the broken system. The good news is that many solutions aren't pie-in-the-sky fantasies; they are practical, data-driven approaches that require shifting from a culture of blame to one of systemic accountability and patient empowerment.
Keep reading with a 7-day free trial
Subscribe to Stephen Thomas BSc (Hons) Substack to keep reading this post and get 7 days of free access to the full post archives.